Fire-Resistant Electrical Standards for Healthcare Facilities
If hospital power fails during a fire, patient risk can change in seconds. In the U.S., medical facilities see about 2,500 fires each year, which is why healthcare electrical work has tighter rules than most buildings.
Here’s the short version: if I’m reviewing hospital electrical fire compliance, I focus on three things first:
- Keep life safety and patient-care circuits running
- Protect rated walls, floors, and ceilings at every penetration
- Make sure generators and transfer switches perform within the required time
That means checking code alignment across NEC Article 517, NFPA 99, NFPA 101, and NFPA 110, then matching those rules to the space:
- Operating rooms: high electrical load, oxygen-related fire risk, strict branch separation
- ICUs: constant life-support loads, dense wiring, heavy equipment movement
- Patient rooms: receptacle wear, cord misuse, added device loads
- Imaging suites: high kVA demand, heat, and routing limits
I’d also verify that:
- Life safety, critical, and equipment branches are assigned and separated the right way
- Metal raceways, CI cable, or MI cable are used where the fire path and code call for them
- Firestopping is listed for the exact field condition, not patched in after the fact
- Generator tests, transfer data, and maintenance records are complete and kept for at least 3 years
- Submittals show the right UL listings, fault ratings, branch use, and installation method before anything is bought
The main point is simple: hospital fire-resistant electrical compliance is not just about picking tougher materials. It’s about keeping power on where patients depend on it, while the building’s fire barriers and backup power system still do their job.
FIRE IN OPERATION THEATRES & ICUs
sbb-itb-501186b
Core U.S. Codes and Standards for Fire-Resistant Healthcare Electrical Systems
Healthcare electrical compliance sits at the intersection of several standards. Each one covers a different part of the job: system design, installation, emergency power, fire barriers, or testing. Put them together, and they focus on three big controls: branch continuity, barrier integrity, and emergency power performance.
Here’s how the main standards split up the work:
| Standard | Primary Scope | Emergency Power | Fire Prevention / Barriers | Inspection & Testing |
|---|---|---|---|---|
| NFPA 99 | Patient care electrical systems; risk categories 1–4; EES design and maintenance | Essential electrical system requirements and generator testing expectations | Risk-based requirements tied to patient care space category | Generator testing logs; EES maintenance records |
| NEC Article 517 | Wiring methods, branch circuits, and power sources for healthcare occupancies | At least two independent power sources; branch separation rules | Metal raceways or metallic-armored cables in patient care spaces | Verification of branch segregation and ground-fault current path integrity |
| NFPA 101 | Building egress, fire detection and suppression, barrier protection, and smoke control | Supports life safety loads such as egress lighting and alarms | Fire-resistance ratings for walls, floors, ceilings; firestopping at penetrations | Barrier inspections; egress lighting and alarm function checks |
| NFPA 110 | Emergency Power Supply System (EPSS) performance, classification, and testing | Level 1 EPSS; transfer and load testing requirements | Keeps life safety systems operational during fire or utility outages | Monthly and periodic load tests; recordkeeping |
| Joint Commission EC.02.05.07 | Utility system management; survey readiness; staff procedures | Emergency power testing and documentation | Labeling of shutoffs; integration with fire alarm and egress systems | Generator logs, transfer time data, and maintenance records |
NFPA 99, NEC Article 517, and NFPA 101 in Day-to-Day Facility Compliance
NFPA 99 sets the risk-based performance target, while NEC Article 517 spells out the wiring methods, branch separation, and load assignment. NFPA 99 groups healthcare spaces by clinical risk - Category 1 through 4 - and ties Essential Electrical System (EES) performance to that risk.
For Category 1 spaces, such as operating rooms and ICUs, the bar is high. These areas require a Type 1 EES with three separate branches: Life Safety, Critical, and Equipment.
Each branch serves a different job. The Life Safety branch supports egress lighting, exit signs, alarms, and other evacuation loads. The Critical branch serves patient care receptacles, operating-room task lighting, and patient-related equipment. The Equipment branch supports HVAC, sterilizers, and other support loads.
NEC Article 517 goes a step further by requiring the Life Safety and Critical branches to stay physically separate. They should not share raceways, junction boxes, or cabinets. In patient care spaces, wiring methods also need to keep an effective ground-fault path, usually through metal raceways or cable assemblies with metallic armor or sheath. In plain terms, this affects how critical-care circuits are routed, divided, and protected.
NFPA 101 provides the building-side rules around all of this. If a conduit, cable tray, or junction box passes through a rated wall, floor, or ceiling assembly, that opening needs a listed firestop system and documented barrier repair. That’s where electrical work and fire barrier work meet, and it’s often where teams get tripped up during installs or later inspections.
NFPA 110 and Joint Commission Requirements for Emergency Readiness
NFPA 110 puts numbers around emergency power performance. For Level 1 systems, emergency power must reach life safety and critical loads within 10 seconds after normal power is lost. That 10-second window is a hard benchmark, not a rough goal.
NFPA 99 also requires 12 load tests each year, spaced 20 to 40 days apart, with each test lasting at least 30 minutes. Facilities should record load, duration, transfer time, and any issues found and fixed. Those records do more than fill a binder. They shape maintenance planning, inspections, and buying decisions.
The Joint Commission's EC.02.05.07 standard connects those code rules to survey preparation. Surveyors review generator logs, transfer-time records, labeling for electrical shutoffs, and corrective action records when tests show problems. They also watch for common paperwork gaps, including incomplete generator test records and improper use of power strips for medical equipment.
Fire-Resistant Cables, Enclosures, and Penetrations in Critical Care Areas
Knowing which code applies is only part of the work. The next part is picking the right materials and putting them in the field the right way. In critical care areas, the wiring method can decide whether a circuit stays alive during a fire. So material choice matters just as much as circuit layout.
Circuit Integrity for Life Safety, Critical, and Equipment Branches
Life safety branch circuits - egress lighting, exit signs, fire alarm detection and notification, elevator controls, and smoke control interfaces - must stay in service for the duration of a design fire, or at least for the required compartment rating. Critical branch circuits that serve operating rooms, ICUs, and life-support equipment must transfer within 10 seconds, which means the feeders have to survive long enough to carry the system through that gap.
In U.S. healthcare work, three wiring methods show up again and again. Each one fits a different part of the building.
| Wiring Method | Fire Performance | Best Fit in Healthcare | Installation Notes |
|---|---|---|---|
| UL 2196 CI Cable | 2-hour circuit integrity and hose-stream test | Fire alarm loops, evacuation circuits, life safety feeders in ICUs and ORs | Flexible routing; suited to survivability routes |
| Mineral-Insulated (MI) Cable | Very high heat tolerance; inherently non-combustible | Main emergency feeders through risers and operating suites | Specialized bending and termination; favored for minimal smoke production and long service life |
| THHN/THWN in Steel Conduit | Relies on building-level fire protection rather than cable-level fire testing | General branch circuits in rated corridors and electrical rooms | Common trade skills; cost-effective; does not provide standalone circuit integrity |
Generator, ATS, and switchboard feeders often run in protected shafts or rated enclosures, subject to AHJ approval.
NEC Article 517 adds another layer in patient care areas: redundant grounding. That means both an equipment grounding conductor and a continuous metallic raceway path are required, which is stricter than standard commercial work. Life safety and critical branches also cannot share raceways, junction boxes, or cabinets with normal power circuits.
And here's the hard truth: even top-tier cable won't help much if the path fails at a wall opening or floor sleeve.
Protecting Rated Walls, Floors, and Ceilings During Electrical Installation
Once the circuit route is set, every penetration turns into a firestop issue.
Any conduit, cable tray, or busway that passes through a rated wall, floor, or ceiling can break the fire barrier. The fix is not generic caulk or field-made patching. It has to be a tested through-penetration firestop system installed to ASTM E814, also referenced as UL 1479.
ASTM E814 assigns two ratings:
- F-rating measures flame and gas spread
- T-rating measures heat rise on the unexposed side
For floor penetrations, the T-rating must be at least 1 hour and no less than the full fire-resistance rating of the floor assembly.
Firestop systems also have to match the exact field condition - the substrate, the penetrating item, and the annular space all matter. A listed system for one penetration type does not automatically work for another. That's why it helps to lock down penetration locations in drawings or BIM before installation starts. Otherwise, crews end up making field fixes, and those fixes can turn into survey deficiencies.
After the barrier is sealed, the next checkpoint is the enclosure itself.
Material Selection for Switchgear, Busway, and Enclosure Components
Hospital electrical rooms need enclosures that can take heat, smoke, and physical abuse - not just carry electrical load.
For switchgear, panelboards, and busway in hospital electrical rooms, steel housings are the baseline. They are the default because they are noncombustible and durable. Inside those assemblies, parts like wire management clips, terminal barriers, arc chutes, and mounting supports should use plastics rated to UL 94 V-0. Those materials self-extinguish and do not drip flaming particles. V-0 is the highest classification in the UL 94 scale, and it is showing up more often inside switchgear and control cabinets for critical care facilities.
Compartmentalized construction helps limit fault and smoke spread. If busway sections, switchgear cubicles, and breaker compartments are split by metallic or fire-resistant barriers, a fault or small fire in one section is less likely to take down the larger distribution system. Electrical rooms should also sit in or next to rated shafts, stay clear of combustible storage, and use non-combustible finishes.
Applying the Standards Across Healthcare Spaces and Maintenance Programs
Fire-Resistant Electrical Standards by Healthcare Space Type
Choosing the right cable and enclosure is only part of the job. In healthcare, fire risk shifts from one space to another. NEC 517 and NFPA 99 set the baseline, but the occupancy type is what drives how far you go with branch separation, feeder protection, and wear-point inspections. Once the code rules and material choices are set, the next move is applying them room by room.
Key Differences Between Operating Rooms, ICUs, Patient Rooms, and Imaging Suites
Operating rooms pack a lot of electrical load into one place. They also bring together an oxygen-enriched atmosphere and active ignition sources like electrosurgical units, lasers, and alcohol-based prep products. That combination makes feeder protection and branch separation the main fire-resistant design concerns.
ICUs create a different kind of pressure. Life-support loads run around the clock through packed headwall wiring, and the steady movement of equipment, plus add-ons over time, can turn cable management into a slow-building fire problem.
Imaging suites bring their own issues. These rooms concentrate very high kVA loads in tight areas, produce a lot of heat from power supplies, and add strong electromagnetic fields that affect routing and shielding decisions.
General patient rooms sit lower on the risk scale, but they still aren't simple. Patient-owned devices, worn receptacles, and overheated cords can still cause small failures that turn into bigger ones.
Use the table below to connect each space with the design control that does the most to cut fire risk.
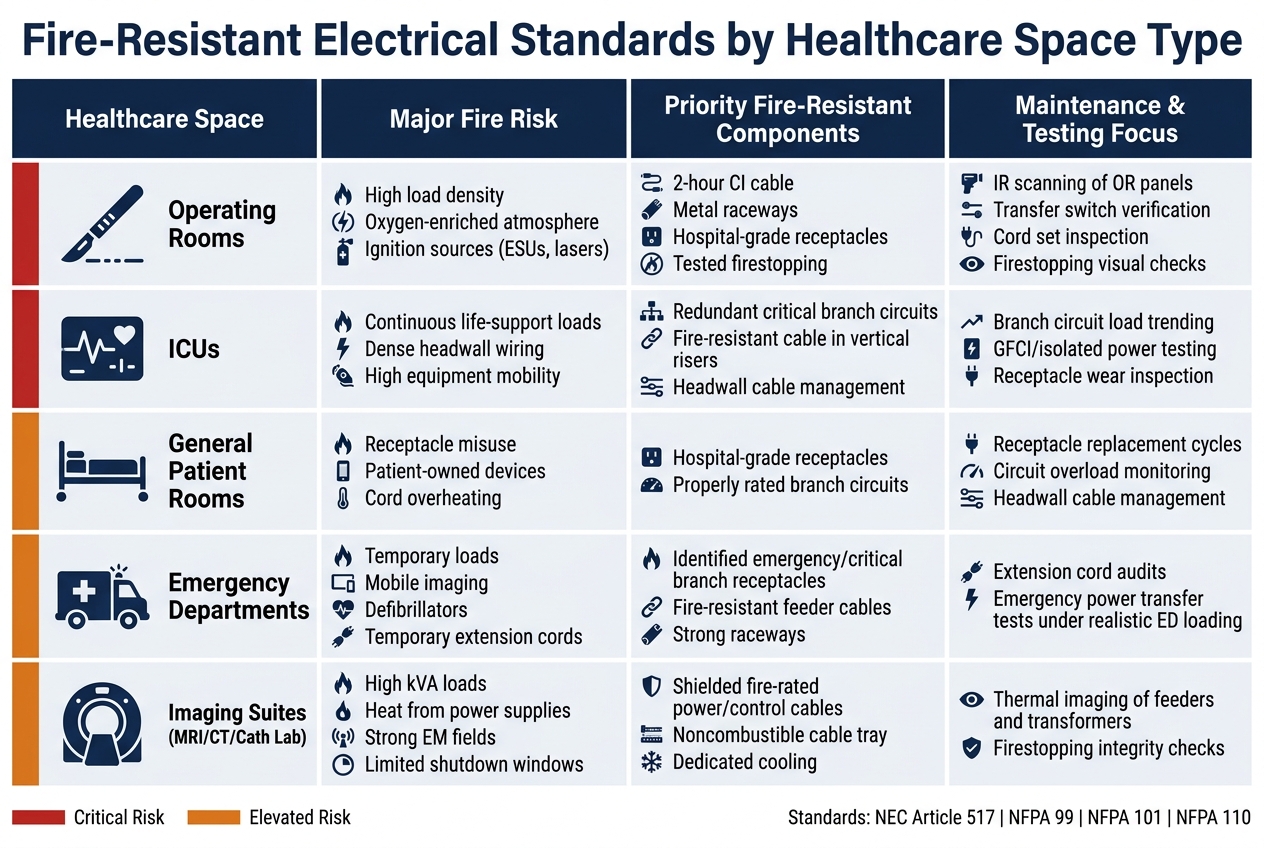
| Healthcare Space | Major Fire Risk | Priority Fire-Resistant Components | Maintenance & Testing Focus |
|---|---|---|---|
| Operating Rooms | High load density, oxygen-enriched atmosphere, ignition sources (ESUs, lasers) | 2-hour circuit-integrity cable or protected routing for life safety and critical branches, metal raceways, hospital-grade receptacles, tested firestopping | Infrared scanning of OR panels, transfer switch verification, cord set inspection, firestopping visual checks |
| ICUs | Continuous life-support loads, dense headwall wiring, high equipment mobility | Redundant critical branch circuits, fire-resistant cable in vertical risers, strong headwall cable management | Branch circuit load trending, GFCI/isolated power system testing where used, receptacle wear inspection |
| General Patient Rooms | Receptacle misuse, patient-owned devices, cord overheating | Hospital-grade receptacles, properly rated branch circuits | Receptacle replacement cycles, circuit overload monitoring, headwall cable management and receptacle condition |
| Emergency Departments | Temporary loads, mobile imaging, defibrillators, temporary extension cords | Clearly identified emergency and critical branch receptacles, fire-resistant feeder cables, strong raceways in high-traffic paths | Extension cord audits, emergency power transfer tests under realistic ED loading |
| Imaging Suites (MRI/CT/Cath Lab) | High kVA loads, heat from power supplies, strong EM fields, limited shutdown windows | Shielded, fire-rated power and control cables, noncombustible cable tray, dedicated cooling for electrical rooms | Thermal imaging of feeders and transformers, firestopping integrity checks in heavily penetrated walls |
Inspection, Testing, and Common Failure Points That Create Fire Risk
Aging breakers are one of the most overlooked hazards in a hospital electrical system. If a breaker does not trip within its rated time, fault current keeps moving, conductors heat up, and insulation starts to fail. In older hospitals, that risk gets worse when protective devices stay in service past the manufacturer's recommended life. NFPA 70B requires risk-based electrical maintenance intervals, torque checks, breaker operation testing, and documentation.
Overloaded circuits often build in a quiet, almost invisible way. New equipment gets tied into old branch circuits, but load calculations never get updated. The result is simple: conductor temperature climbs, insulation wears down, and the system keeps getting weaker until something gives way.
Missed post-project firestop inspections are another common weak spot. One new cable run through a rated wall without a listed sealant - or even one sleeve left open after a job - can break the compartmentation plan that NFPA 101 relies on. In clinical spaces, every electrical penetration should be checked after project work. That step shouldn't be optional.
Emergency power has its own paper trail for a reason. Written records of all inspections and tests must be kept for at least 3 years. If those intervals are missed, it is not just a code issue. It also means the generator or transfer switch may fail at the exact worst moment.
Build these checks into procurement specs, work orders, and CMMS schedules so the design team, installers, and maintenance staff are all working from the same playbook.
Procurement and Key Takeaways: Specifying Compliant Equipment for Healthcare Projects
Vague purchase specs leave room for compliance problems. Procurement is the last point where you can lock in branch class, ratings, and listing rules before anything gets installed. And the same three controls used throughout this guide still matter here: branch continuity, barrier integrity, and emergency power performance.
Standards-Based Equipment Specifications for Purchasing Teams
Write submittals to the adopted code editions, required UL listings, and AHJ amendments. Don’t rely on loose wording like “meets the adopted code editions and listed product requirements.”
Before any component is approved, confirm which branch it serves - life safety, critical, or equipment - because NEC Article 517 applies different rules to each one. That branch class should be plainly shown in the submittal package.
Use the same branch and rating terms from design review in every submittal and purchase order. Here’s the purchase-stage check for each main component:
| Component | Required Listings and Ratings | Common Healthcare Applications | Purchase-Stage Checks |
|---|---|---|---|
| Breakers | UL 489 or UL 1066 listing, interrupting rating, selective coordination data | Life safety and critical branch panelboards, patient care feeders | Verify listing, match fault rating, confirm coordination study |
| Transformers | Insulation class, temperature rise, enclosure type, fire-rated room requirements | Step-down distribution, isolated power systems, imaging suite loads | Verify listing, confirm enclosure type, match heat load to room rating |
| Switchgear/Switchboards | UL 891 or UL 1558 listing, short-circuit/withstand rating, enclosure compartmentalization | Main distribution, essential electrical system segments | Verify listing, match fault rating, confirm compartmentalization |
| Generators & Transfer Switches | NFPA 110 compliance, fuel endurance, transfer switch listing | Emergency power for life safety and critical systems | Verify NFPA 110 listing, confirm fuel endurance rating, match transfer switch to branch load |
| Fire-Resistant Cable Assemblies | UL 2196 circuit-integrity listing, 2-hour fire-resistance rating, approved support method | Life safety circuits, emergency feeders, critical care branch wiring | Require the listed cable-and-support assembly approved for the route |
If a submittal can’t prove the listing, rating, and installation method, reject it before release. Simple as that.
Electrical Trader is one sourcing option for breakers, transformers, switchgear, and power generation equipment. But the source doesn’t change the review standard. Every item, from every channel, should go through the same submittal and documentation check. Require proof of listing, service history for used gear, and confirmation that ratings match the fault study before installation.
That language should appear in every healthcare purchase order.
Key Points for Design Reviews, Retrofits, and Replacement Planning
For retrofit and replacement work, confirm which code editions the AHJ has adopted. Don’t assume the version used when the building first went up still applies. Replacement equipment must match the branch class, ratings, and enclosure type of the gear it replaces, and purchase approval depends on matching the existing system’s listed installation method. If there’s any change, get written engineering approval.
Treat documentation completeness as a pass/fail item. If a manufacturer can’t produce the exact listing report, installation method, or testing schedule required for the job, the product should not be approved - no matter how well known the brand may be.
Build acceptance testing, periodic generator tests at the required intervals, firestop inspections, and replacement planning into procurement contracts from day one. That way, maintenance staff gets a complete compliance record instead of a folder full of holes.
FAQs
Which healthcare spaces need the highest fire-resistant electrical protection?
Category 1 spaces need the highest level of fire-resistant electrical protection. This group includes operating rooms, intensive care units, emergency departments, and cardiac labs. In these areas, a power failure can put patients at the highest risk of severe injury or death.
Because of that, these spaces require Level 1 emergency power systems. That setup includes dedicated fire-rated rooms with a 2-hour rating for the emergency power supply and its supporting equipment.
How do I know if a firestop system is listed for the exact penetration condition?
Check the entire assembly against the manufacturer’s UL FHIT documentation, not just the parts on their own. The listing needs to match your exact circuit type, wall or floor build, and the way the system is installed.
In the U.S., compliance depends on the complete system. That means the raceways, supports, fittings, and firestop materials all need to line up with the listed assembly. It’s also smart to confirm any project-specific requirements with your local AHJ.
What documents should a hospital keep to prove generator and transfer switch compliance?
Hospitals should keep complete, accurate on-site records for at least 36 months.
Key documents include:
- operational logs
- monthly generator test results
- fuel quality reports
- battery maintenance records
- transfer switch (ATS) logs, including transfer times
Skip vague notes like “pass” or “OK.” Those entries don’t tell you much when you need to track a problem or show what happened during an inspection.
Instead, record the actual measured data, the date, who did the work, any unsatisfactory conditions, and the corrective actions taken.